
Introduction
Surgical units operating within a tertiary hospital perform thousands of operations every year comprising a mix of elective and emergency surgery. These operations occur in operating theatres and endoscopy suites, with various anaesthesia modalities ranging from general anaesthetic administered by an anaesthetist to local anaesthetic without sedation administered by the operating clinician (LA-only). In accordance with our ethical responsibilities as clinicians, we strive to meet the patient’s needs by providing healthcare based on wise and cost-effective management of limited clinical resources.1 Health service providers have an ethical and financial responsibility to provide care to the patient that meets their care needs but is also cost-effective. Efficient use of limited health resources allows more patients to receive care.
In response to the COVID-19 pandemic, when there were many barriers to operative management, the Northern Hospital plastic surgery unit instituted a practice of using spare operating theatres for LA-only procedures to help manage the burden of operative trauma in an environment where access to fully staffed operating theatres was reduced. A surgical registrar and a resident would prepare a sterile scrub trolley, open and count instruments, and perform the procedure without the usual theatre staff in attendance. The patient would walk from the day surgery unit or the emergency department to the operating theatre and depart in the same fashion. Procedures were undertaken on weekdays during business hours when a supervising consultant was available.
The preliminary success of this approach led to the establishment of a funded minor procedure room with surgical instruments, a diathermy machine, suction and all the additional consumable equipment required to perform sterile operations (see Figure 1). A one-time set-up cost of approximately AU$12,000 was required to facilitate a fully operational minor procedure room. The establishment and maintenance of this room was under the responsibility of the plastic surgery nurse practitioner.

Wide-awake local anaesthetic, no tourniquet surgery (WALANT) and LA-only surgery have been shown to be safe and cost-effective methods of delivering elective surgery in the United Kingdom2 and United States of America,3 with established LA-only operating theatre facilities delivering streamlined care to a subgroup of appropriate patients. No previous studies have reported on the use of dedicated LA-only emergency surgery and no Australian centres have reported the implementation of LA-only surgery within a dedicated minor procedure room. The status quo in Australian public and private hospitals is that patients who require operative care undergo their procedures in formal operating theatres with a full complement of staff.
This paper aims to review the preliminary success of applying an LA-only approach to emergency surgery, including the estimated economic benefits, and discuss some associated pitfalls.
Methods
From February 2022 until December 2022, LA-only procedures were undertaken in a minor procedure room or an unused operating theatre. Patients included were aged 18 to 88 years. Any cases involving anaesthetic or theatre nursing staff were not included.
Data was collected contemporaneously as part of the unit’s clinical governance and audit processes. The on-call consultant ultimately took the decision to perform a case in the minor procedure room on the day of presentation.
Measured outcomes included complications and procedure failure requiring planned repeat procedures in an operating theatre. Complications were defined as surgical site infection or unplanned return to operating theatre.
Estimated per-hour costs were calculated according to staff wages and do not account for consumables. Staff wages were calculated from the relevant enterprise bargaining agreements (EBA) from the Australian Fair Work Commission.4–6 Wages for an individual job title can vary depending on the experience and role classification in the EBA. Where a pay range exists for a particular role, the median value was used for estimation. Wages were calculated using standard in-hours pricing and do not account for after-hours or weekend rates.
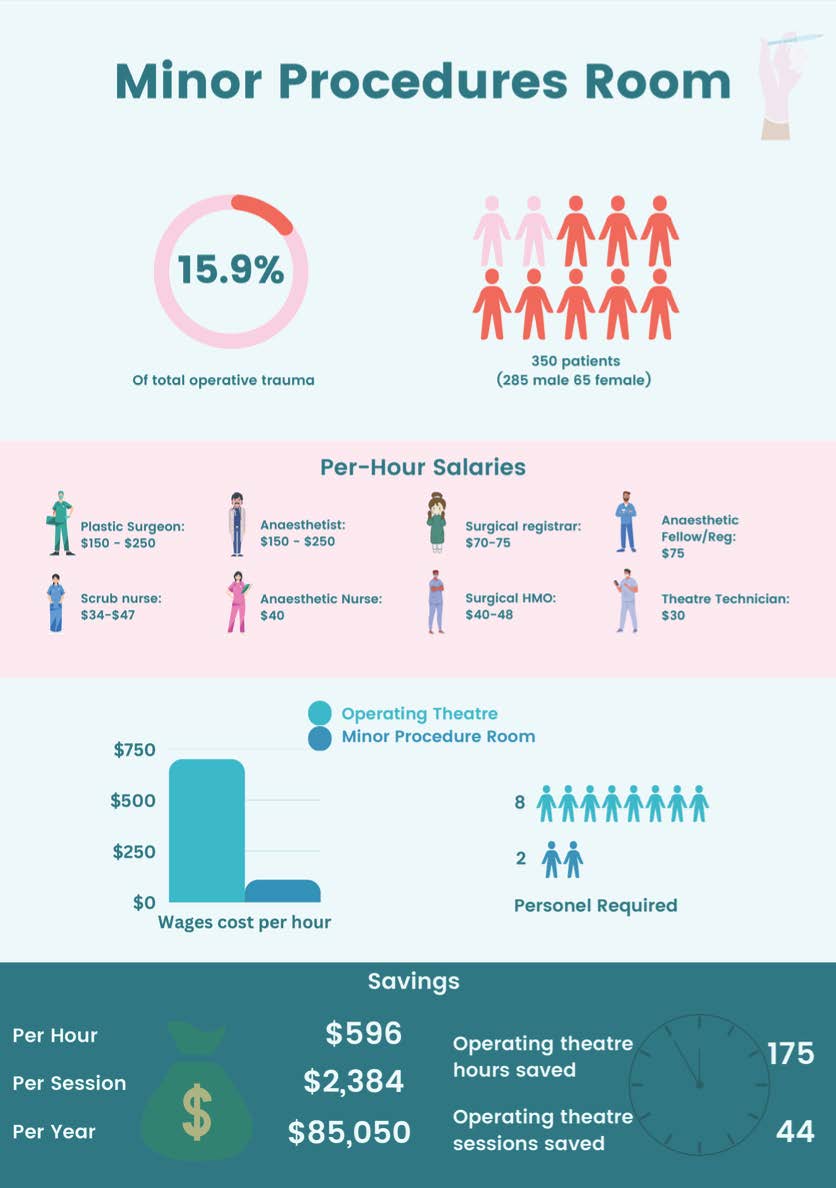
Operating theatre costs account for one consultant anaesthetist, one anaesthetic registrar/fellow, one anaesthetic nurse, two theatre nurses, one theatre technician, one consultant surgeon and one SET trainee. Costs for the minor procedure room account for one unaccredited registrar and one resident/hospital medical officer.
Case duration was defined as the time from when the patient was called for until the surgical staff were ready to call for the next patient. The estimated duration of the minor procedure room case was one hour. To estimate total theatre sessions saved, cases performed in the main operating theatre were assumed to be carried out twice as fast compared to the minor procedure room. This assumption is due to the additional staff in the main operating theatre facilitating a faster turnover of cases. In our calculation, a theatre session was set at four hours.
Quality assurance approval was obtained from the Northern Health Research Ethics Department before the commencement of the study (ALR No 31.2023).
Results
Demographics
Overall, 350 patients (285 males and 65 females) underwent LA-only operations in the minor procedure room (see Figure 2).

The mean age of patients was 42. There were 309 hand/upper limb cases, 31 general plastic surgery cases, two elective skin cancer excisions and eight lower limb cases. The two elective cases were moved ad hoc to the minor procedure room to free up space in the main operating theatre. There were no complications and no procedure failures (see Table 1). Data was not available for wait times for patients undergoing minor procedures.
In the same period, the unit performed 1857 cases in a staffed operating theatre with an average wait time of 15 hours from booking until operation. Of 2207 emergency operations, 350 (15.9%) were performed in the minor procedure room.
Savings
The hourly cost to perform procedures in the minor procedure room is approximately AU$110 in staff wages. The hourly wage to run a fully staffed operating theatre is approximately AU$700 in staff wages, and the sessional cost is approximately AU$2800.
Overall, 350 cases performed in a minor procedure room saves approximately 44 fully staffed theatre sessions per year, assuming cases performed in a minor procedure room could be done twice as fast in the main operating theatre.
With the above estimates, a procedure room saves AU$596 per hour, AU$2384 per session and AU$85,050 per year. See Supplementary material 1 for a savings calculator.
Discussion
This paper demonstrates that a minor procedure room for LA-only emergency operations has notable benefits.
Hospital benefits
A hospital using a minor procedure room generates significant gross cost savings. Even when accounting for initial set-up costs, estimated at AU$12,000, and for error or overestimation, the cost savings are still significant, with savings being realised within a single quarter. This study likely underestimates cost savings as the calculation does not use after-hours and overtime rates. In reality, many cases undertaken in the minor procedure room would otherwise need to be conducted after-hours in the main operating theatre at elevated staff pay rates.
Patient benefits
Patient waiting times for emergency surgery are reduced for patients undergoing surgery in operating theatres as well as patients in the minor procedure room. While staff are operating in the minor procedure room, other staff can operate in standard operating theatres, thus increasing the efficiency of the unit. While specific data for waiting times for patients undergoing minor procedures is not available in this study, patients deemed suitable for LA-only surgery and referred before 15:30 on a given day generally received their care on the same day. In a busy tertiary hospital unit performing nearly 2000 emergency procedures in the main operating theatres, saving at least 44 emergency operating sessions (176 hours) is significant.
With appropriate patient selection, performing LA-only surgery is safe. Patients who agree to have their operation in the minor procedure room forego the option of sedation at the time of surgical consent. This potentially results in a lower sedation administration rate than would occur if the patients had their procedures in an operating theatre.
Clinician benefits
Having an additional clinical domain to deliver care means junior staff get more exposure to primary operating. Compared to the alternative—where multiple junior staff may be clamouring for operative experience in a single theatre staffed with a consultant and a surgical trainee—the addition of a minor procedure room allows unaccredited registrars and residents to gain clinical experience in running an emergency list, administering local anaesthetic and performing simple procedures with onsite consultant supervision. Furthermore, the junior staff who run a minor procedure room are responsible for all aspects of managing the list in addition to the standard surgical responsibilities, including counting and scanning sterile equipment, cleaning the room between operations, and sterile trolley set-up. For this reason, we defined case duration as the time from when the patient was called for until the surgical staff were ready to call for the next patient. Exposure to these aspects of running a surgical operating list, which generally fall into the domain of theatre technicians and nurses, is valuable as it gives junior staff a deeper understanding of all the moving parts that make up an operating list.
Patient selection
In addition to the obvious benefits of a minor procedure room, there are also risks and pitfalls. The operation of a minor procedure room is dependent on appropriate patient selection. Patients need to be compliant, ambulant, free from infectious diseases requiring contact/airborne precautions and sufficiently stoic to cope with the pain of local anaesthetic administration. Even when patient factors are optimal, the presenting injury also needs to be considered. An injury that requires prolonged tourniquet time, microsurgical repair, intraoperative X-ray or significant proximal extension of the incision is unlikely to be successfully carried out in the minor procedure room. Appropriate patient selection is facilitated by thorough clinical history, with particular attention to the mechanism of injury. Explicit explanations of the rigours of the administration of local anaesthetic are a necessary part of consent for patients who will be treated in the minor procedure room.
While there were no procedure failures in our cohort, inappropriate patient selection resulting in an unexpected intraoperative finding can result in procedure failure or a prolonged procedure. In the event that an unexpected intraoperative finding requires senior staff assistance, the time-saving benefits of operating in the LA-only minor procedure room are potentially lost as senior staff are drawn away from the main operating theatre to assist.
Adverse events
There were no adverse events in our cohort. In the event of local anaesthetic toxicity, anaphylaxis or a patient becoming unresponsive during a procedure, the minor procedure room is not optimally located for swift response by critical care staff. Unlike the emergency department or the operating theatre complex, which have specific processes and alarms for dealing with critical patients with critical care staff nearby and available, the minor procedure room is situated on a ward. If a patient becomes unresponsive, a standard ward code would need to be called. This minor trade-off relates to the practicality of the location of the available room dedicated as the minor procedure room in our hospital. If a minor procedure room was to be set up in another facility, we recommend mitigating the risk of adverse events by locating the procedure room adjacent to the operating theatre complex, intensive care unit or emergency department.
Clinical infrastructure
In addition to the room itself, other clinical areas are required for the functional operation of a minor procedure room. An admissions area or day procedure unit is required to clerically and clinically admit and discharge patients. This occupies resources that are usually allocated to the operating theatre complex. It can be argued that this cost is not an actual added cost as these patients would nonetheless require an operating theatre in the absence of a minor procedure room. Patients can be escorted from the emergency department and brought directly to the minor procedure room if the timing is opportune.
Clinical governance
Unlike a standard operating theatre where nursing staff record many clinically crucial key performance indicators using internal hospital software, this data is not captured in our minor procedure room. As a result, procedure lengths are estimated, and Medicare benefit numbers are not coded at the time of the procedure but are left to be coded by the medical records department. The minor procedures are not booked, recorded or carried out in the same way as emergency operating theatre cases and are therefore not visible to hospital executive staff in the same way. The unit keeps the record of minor procedure room operations in a running contemporaneously updated spreadsheet. This process is a deviation from standard clinical governance and workflow management and does not capture the unit’s workflow in a way that is viewable to the hospital executive. It also may result in the hospital under-reporting its operating activity and potentially not optimising its funding from the government. This problem can be mitigated by changing clinical workflow systems or by further collaboration of clinical and executive staff.
The incomplete clinical governance surrounding the minor procedure room also precludes another potentially monumental cost saving of booking LA-only elective surgery cases. Our facility cannot schedule elective LA-only cases in the minor procedure room. This is an area for further exploration, improvement and innovation.
Conclusion
When implemented and managed appropriately, a minor procedure room for LA-only emergency surgery can generate significant cost and time savings for a hospital. This model’s benefits outweigh its pitfalls and has been successful in our institution. Other centres are likely to benefit from the implementation of a plastic surgery minor procedure room.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Acknowledgement
The authors would like to acknowledge the contribution of economist Ben Grodeck.
Revised: July 13, 2023 AEST; November 12, 2023 AEST