


Introduction
Head and neck defects are reconstructive challenges, demanding functional restoration of speech, swallowing and airway maintenance. When free tissue transfer is required, consideration should be given to sufficient pedicle length, flexibility for reconstruction of complex contours, such as the ear and nose, and functional requirements. A thin fasciocutaneous flap with the option to incorporate fascia, muscle or bone, with minimal donor site morbidity, is ideal. Current workhorse flaps in head and neck are limited by donor site morbidity or tissue bulkiness. This has encouraged the search for alternatives; supported by recent advances in microsurgery and new perforator flaps exploiting understanding of the angiosome and perforator anatomy.1,2 The superficial circumflex iliac artery perforator (SCIP) flap, first described by Koshima in 2004, represents an excellent alternative to traditional flap options.3
The SCIP flap is commonly raised as an axial pattern flap, based on the superficial circumflex iliac artery (SCIA) that travels from the origin of the vessel towards the anterior superior iliac spine in most cases. Its pedicle travels in the plane superficial to Scarpa’s fascia, running parallel to the deep circumflex iliac artery (CIA), which provides the pedicle for the traditional groin flap described by McGregor and Jackson.4–7 The anatomy of this flap is well described by Berner and colleagues.7 The SCIP flap has many advantages including an inconspicuous donor site that closes directly, a relatively short raise time, thin and pliable fasciocutaneous tissue, pedicle length and options for chimeric flap design. Despite these advantages, recent investigation into its use is relatively low volume. The SCIP flap has been successfully used for reconstructing various head and neck defects, including pharyngeal, buccal, floor of mouth, osseocutaneous reconstructions and cutaneous resurfacing.5–9
In this study our aim was to describe our institutional experience with using the SCIP flap to reconstruct head and neck defects including, to our knowledge, the first published reports of using the SCIP flap for nasal reconstruction and partial auriculectomy.
Methods
A retrospective review of head and neck reconstruction using the SCIP flap at our institution from 2019 to 2020 was undertaken. The study includes 11 patients undergoing head and neck reconstruction with 12 SCIP flaps. All patients provided informed consent to surgery and for publication of clinical images. Ethics approval was given by the South West Sydney Local Health District Ethics Committee (approval number 2022/STE03301). Patient demographics, indications for reconstruction, operative details, flap survival and complications are reported. All patients were operated on by a single surgeon (CA, senior author).
Preoperative planning and assessment
Computed tomographic angiography was performed to identify suitable anatomy in addition to duplex ultrasound mapping of bilateral SCIAs (Figure 1A). Selection of side was made based on anatomy of the SCIA, vessel calibre and pedicle course. For the most recent patients in our series, duplex ultrasound mapping by a qualified sonographer was introduced as a supplementary imaging modality to aid preoperative planning (Figure 1B). The flap template, femoral vessels, superficial branch of the CIA and point at which the SCIA perforated the deep fascia were marked on the patients’ skin prior to operation.
_on_table_duplex_imaging_and_resulting_scia_mapping_pe.png)
Surgical technique
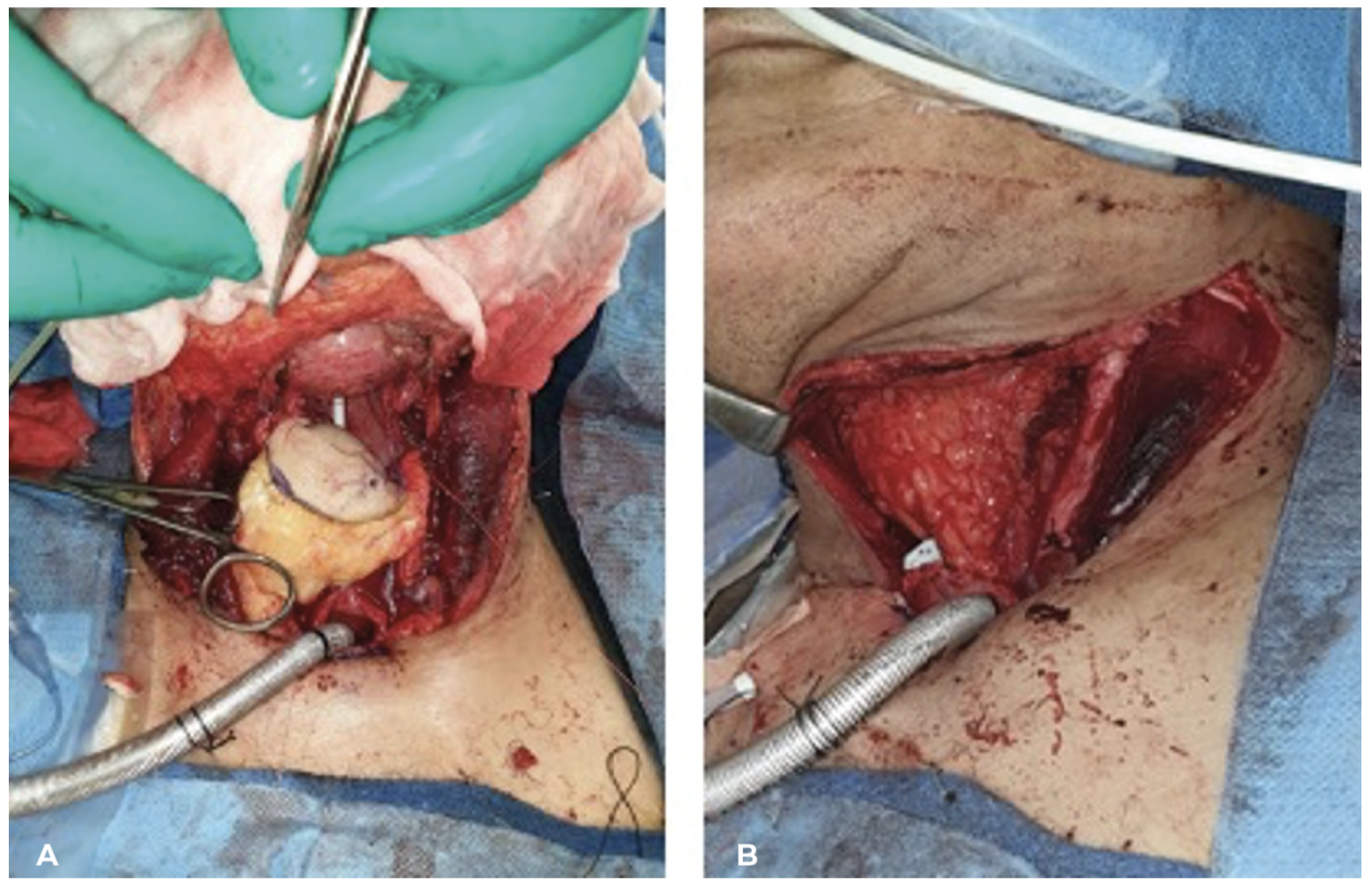
Flap raise proceeded as previously described.6 The inferior and lateral skin incisions were made to raise laterally. Dissection proceeded from lateral to medial in the plane superficial to Scarpa’s fascia and was informed by markings based on duplex imaging until the candidate perforating superficial branch was identified. A 4-point static lone star retractor (Endotherapeutics, Epping, NSW, Australia) aided this part of the dissection. In all cases, the superficial circumflex iliac vein (SCIV) was identified and preserved. To obtain additional pedicle length and better vessel calibre size, dissection of the perforating branch was continued through the deep fascia at the area of perforation to the origin from the femoral artery with the aid of assistant retraction. The termination of the SCIV or the vena comitans of the SCIA were also dissected through the deep fascia up to the saphenofemoral junction to provide maximum pedicle length and vessel diameter. The deep branch of the superficial circumflex iliac system was identified and ligated using surgical clips, and flap perfusion was verified on-table. Where multiple perforators were identified during dissection, preservation of encountered perforating vessels was undertaken until a candidate axial SCIA or dominant direct anchoring perforator could be positively identified. Where the flap design was modified to include a ‘mini-SCIP’ flap monitoring paddle, its perforator was preoperatively identified by duplex and hand-held Doppler and dissection carried out in a ‘free-style fashion’, tracing the perforator back to its communication with the SCIA to allow a chimeric design double skin paddle flap (Figure 2 and Figure 3). Microsurgical anastomoses were performed end-to-end or end-to-side using 9-0 or 10-0 nylon, and venous couplers (2–2.5 mm size) were used for the venous anastomoses. The donor site was closed directly in layers over a 10F Jackson–Pratt suction drain. A Prevena incisional negative pressure dressing (Acelity, San Antonio, Texas, USA) was applied to the donor site.
_on_table_dup.png)
_inset_as_.png)
Postoperative care
Flaps were monitored by clinical observation and hand-held Doppler where the skin paddle was exterior and accessible. Where the flap was buried, as in the laryngeal reconstructions, a mini-SCIP skin paddle was externalised for monitoring if possible and an adjunct Cook implantable Doppler (Cook Medical, Bloomington, Indiana, USA) was used to monitor the flap arterial flow for a period of five days. Patients received perioperative intravenous antibiotics and 5000 units twice daily of subcutaneous heparin prophylaxis, plus 100 mg of aspirin daily which continued for six weeks. The donor site incisional negative pressure dressing was removed at one week. Suction drain remained until output weaned below 30 ml a day for two consecutive days.
Results
Demographics
From 2019 to 2020 we performed 12 free SCIP flaps in 11 patients at our institution. Cohort demographics are presented in Table 1. Most were male, ASA (American Society of Anaesthesiologists) status III and had an average body mass index (BMI) of 26. Comorbidities are as listed; most were current or ex-smokers. All patients underwent ablative surgery for malignancy—squamous cell carcinoma in eight of 11 patients; melanoma, myofibroma and chondrosarcoma in the remaining three. Patients in the series were followed for a mean of 202 days.
Operative and flap characteristics
The indications for reconstruction were five salvage laryngectomies, four cutaneous defects and two oral cavity defects (Table 2). Our series included the reconstruction of a subtotal auriculectomy and a total nasal defect post rhinectomy. We performed SCIP reconstruction in seven patients who had previous radiotherapy, while three patients underwent adjuvant postoperative radiotherapy and two patients required no radiotherapy. The mean flap area was 92 cm2, with average width and length presented in Table 2. All flaps were raised on a single perforator and vascularised using a single artery and vein at initial flap transfer. The mean flap raise time and ischaemic time was 58 minutes and 85 minutes, respectively.
Complications
Complications are presented in Supplementary material 1, with four patients requiring return to theatre. There were two salvaged microvascular complications, one arterial and one venous. Venous insufficiency occurred in the reconstruction of a total rhinectomy, requiring vein grafting onto the superficial temporal vein and resulting in flap salvage with partial necrosis. Arterial insufficiency was encountered following reconstruction of the hemiglossectomy defect, which was identified immediately postoperatively and salvaged with vein graft. Two patients receiving SCIP reconstruction for salvage laryngectomy defects had early salivary leak and required reoperation.
Discussion
The SCIP flap is now an established option for the reconstructive surgeon.6 Most reports using SCIP flaps for head and neck reconstruction are limited6,7 but evolving.8 In practised hands, it can be raised in a brief period with average raise times as low as 45 minutes.6 The average raise time in this series was comparable at 58 minutes (Table 2). A donor site distant from the head and neck facilitates a two-team approach, allows for concurrent raise, and has the potential to further reduce total operative time and associated risks. Another attractive feature of the SCIP flap is its tissue thickness and pliability, regardless of body habitus. In our series the SCIA was frequently travelling at a depth of less than 1 cm, a finding consistent with published reports.5 When the patient’s body mass index is lower, as often is the case for head and neck cancer patients, the flap can be extremely thin. A thin flap offers flexibility without unnecessary bulk and folds without significant flap compromise. This feature was exploited in the series presented here, to provide double-breasted pharyngeal repairs, nasal lining and auricle reconstruction.
The donor site is a clear advantage of the SCIP flap over other fasciocutaneous flaps used in head and neck reconstruction.10,11 It is concealed, relatively hairless, and closes primarily depending on skin paddle size. Our largest flaps were 20 cm in length and 7–8 cm in width, and primarily closed. Adjunct techniques described to ensure complication free donor site healing include creative postoperative bandaging and incisional negative pressure dressings.12,13 We routinely employed the use of incisional negative pressure as previously described and encountered only a single minor wound dehiscence that healed with conservative measures.12 Pedicle length has been suggested as a disadvantage of the SCIP flap, but our experience was in most cases to the contrary. To ensure an additional 2–3 cm of pedicle length, the SCIA and SCIV can be traced to their origins on the femoral vessels. Only in our case of tongue reconstruction did we have trouble due to inadequate length, as discussed below.
Laryngeal reconstructions
Reconstruction after salvage laryngectomy is challenging, with primary chemoradiation creating an inhospitable wound healing environment. Pharyngeal stricture, anastomotic leak and pharyngocutaneous fistula are the key operative complications a reconstructive surgeon must overcome.14 Although some defects may have adequate remaining tissue for direct closure, poor wound healing in salvage laryngectomy leads to unacceptably high complication rates with primary closure alone.15 Several approaches to address this apply the principal of pharyngeal interposition graft. The most accessible is onlay pectoralis major flap.16 However, high rates of anastomotic leak, stricture, neck stiffness, upper limb mobility restriction and cosmetically unfavourable results are associated with this reconstructive technique.14 In our institution, pectoralis major flaps are used only as a salvage technique for failed free tissue transfer and as a primary procedure reserved for medically infirm patients. Microsurgical transfers provide many options for vascularised non-irradiated tissue and are the first line for pharyngeal defects, with radial forearm and anterolateral thigh flap being the most widely reported. The main advantage of the SCIP flap is that the thinness allows for ease of tube formation even in obese patients (where anterolateral thigh flap may be too thick or radial forearm flap too small of a surface area for tube formation). The other alternative in this setting would be a free jejunal flap, with the associated donor site morbidity and inability to co-raise. The series presented here represents to our knowledge the largest single series of pharyngeal reconstructions using the SCIP flap with five cases. Squamous cell carcinoma (SCC) was the primary diagnosis for all pharyngeal reconstructions in our series. Indications for salvage laryngectomy were: recurrent SCC, primary SCC not suitable for organ-sparing systemic therapy, chondrosarcoma in the setting of definitive radiotherapy, recurrent SCC with chondroradionecrosis and isolated chondroradionecrosis. A double-breasted technique was used. Skin was inset to the pharyngeal defect and a folded, de-epithelialised, redundant portion of flap sutured over the top to provide a double-layered repair, a tactic associated with reduced complication rates for other fasciocutaneous pharyngeal reconstructions.17 All pharyngeal reconstructions presented here survived; although in our series, a high proportion (two of five or 40%) of cases experienced early salivary leak and required salvage procedures, including remobilisation, inset of the flap and reinforcement with pectoralis major muscle tissue. At the time of follow up and most recent speech pathology review, there were no pharyngocutaneous fistulae and all patients were tolerating, at minimum, a soft diet, had adequate swallow and were trialling voice prosthesis. Salivary bypass with Montgomery tube and further modification as instructed by studies of laryngeal reconstruction with other fasciocutaneous flaps will help achieve the lowest possible rates of fistula and stricture long-term with the SCIP flap.18
Oral reconstructions
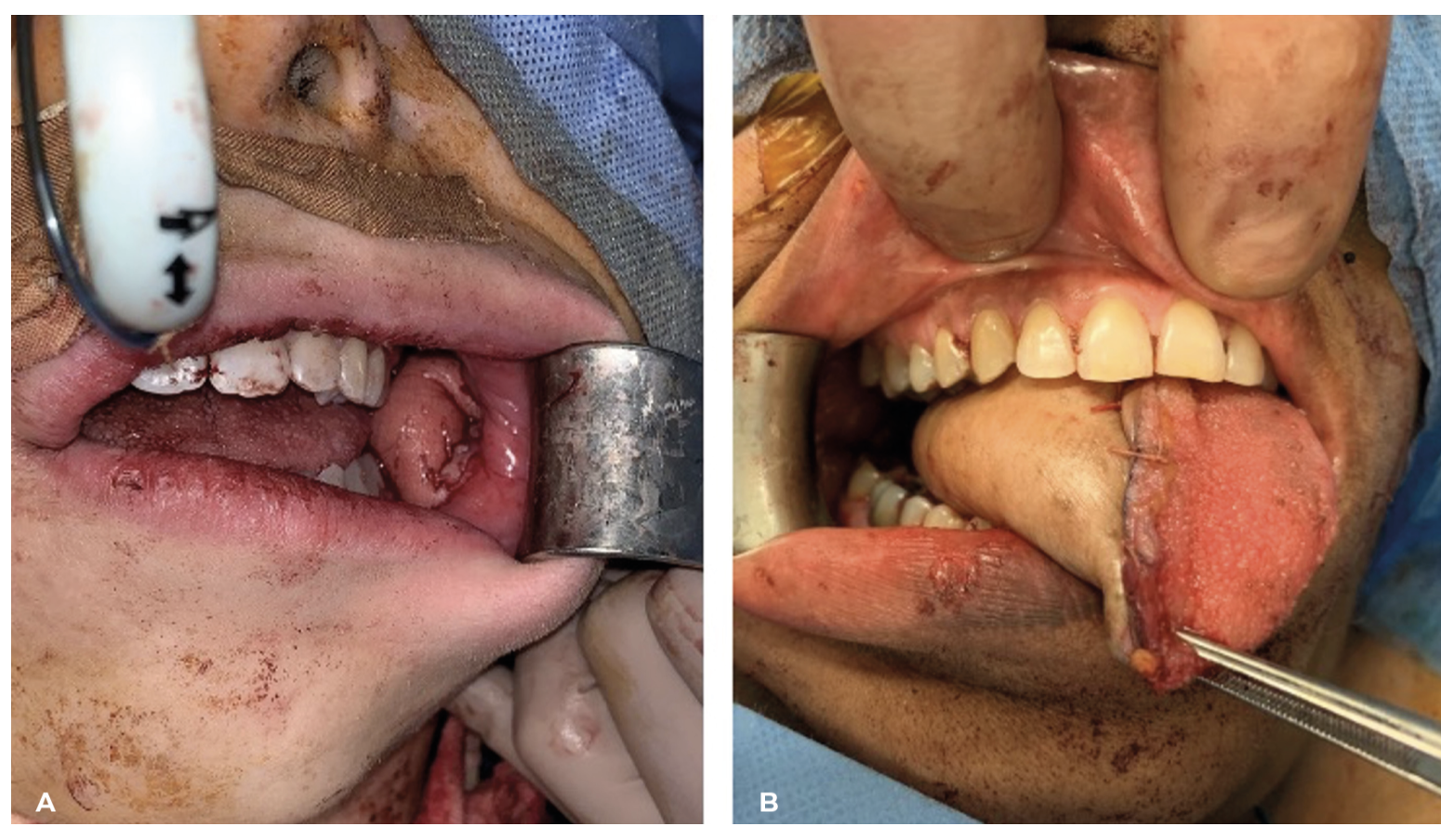
In oral reconstruction there are a myriad of free tissue transfer options available to the reconstructive surgeon, largely owing to the high variability of defects and the precise nature of the reconstructive task. Common defects include the floor of mouth, tongue and buccal mucosa. The SCIP flap has been previously described for each of these.8,19–21 In our series we reconstructed a buccal defect in a patient that presented relatively little challenge (Figure 4A). The reconstruction was well suited, with adequate pedicle length to reach the facial vessels as recipients, and tissue thinness provided an ideal fit without excess bulk to interfere with mastication. Discussion in the reports of buccal mucosal defect reconstruction using SCIP flaps provides similar insight.19,22
_buccal_mucosal_reconstruction.png)
The tongue represents a challenge for the reconstructive surgeon, with functional tongue reconstruction continuing to elude us. Providing adequate, pliable fasciocutaneous reconstruction and minimising scar contracture or tethering to provide optimal speech and swallow are the reconstructive goals.23 The radial forearm and anterolateral thigh are the typical workhorse flap for intraoral reconstruction however both options have their limitation.24 We considered the SCIP flap as an alternative, with the added benefit of a more favourable donor site. Published literature for SCIP flaps in tongue reconstruction offers favourable reports in the setting of glossectomy (see Supplementary material 2), including a series of nine cases published by Ma and colleagues, who reported no issues with pedicle length or any significant technical difficulties.20 In our experience the pedicle length presented a challenge to reach vessels in the neck. We inset prior to microsurgical anastomosis and the pedicle was tunnelled through the neck (Figure 4B). This required technically very difficult microsurgery and ultimately a small inferior border mandibular ostectomy (2 × 1 cm) was required to facilitate the anastomosis which was deep to the inferior mandibular border due to short pedicle length. In hindsight, performing the anastomosis in the neck first and tunnelling the flap through the floor of the mouth to the defect secondarily may have made the technique easier, although significant care would be required to avoid tension on the anastomosis during this manoeuvre.
Cutaneous reconstructions
Our cutaneous reconstructions included a rhinectomy, auriculectomy and skin resurfacing of the neck of a salvage laryngectomy patient (Figure 5). A subtotal auriculectomy was undertaken as a wide local excision for melanoma. The partial auriculectomy spared the helical root and superior helix, with the resultant defect requiring reconstruction of the anterior and posterior aspect of the ear. The pliability of the SCIP flap allowed for folding of the flap and inset to reconstruct both aspects and maintain the external auditory canal (Figure 5C). A report by Koshima’s group has previously described the use of SCIP flaps for reconstruction of the canal after tumour extirpation requiring temporal bone resection.25 Our patient is currently healed and is under consideration for a second stage debulking and insertion of cartilaginous framework to provide a more anatomically accurate and cosmetically acceptable result. In future it will be exciting to see how the SCIP flap can be applied to multistage ear reconstruction.
_frontoethmoidal_reconstru.png)
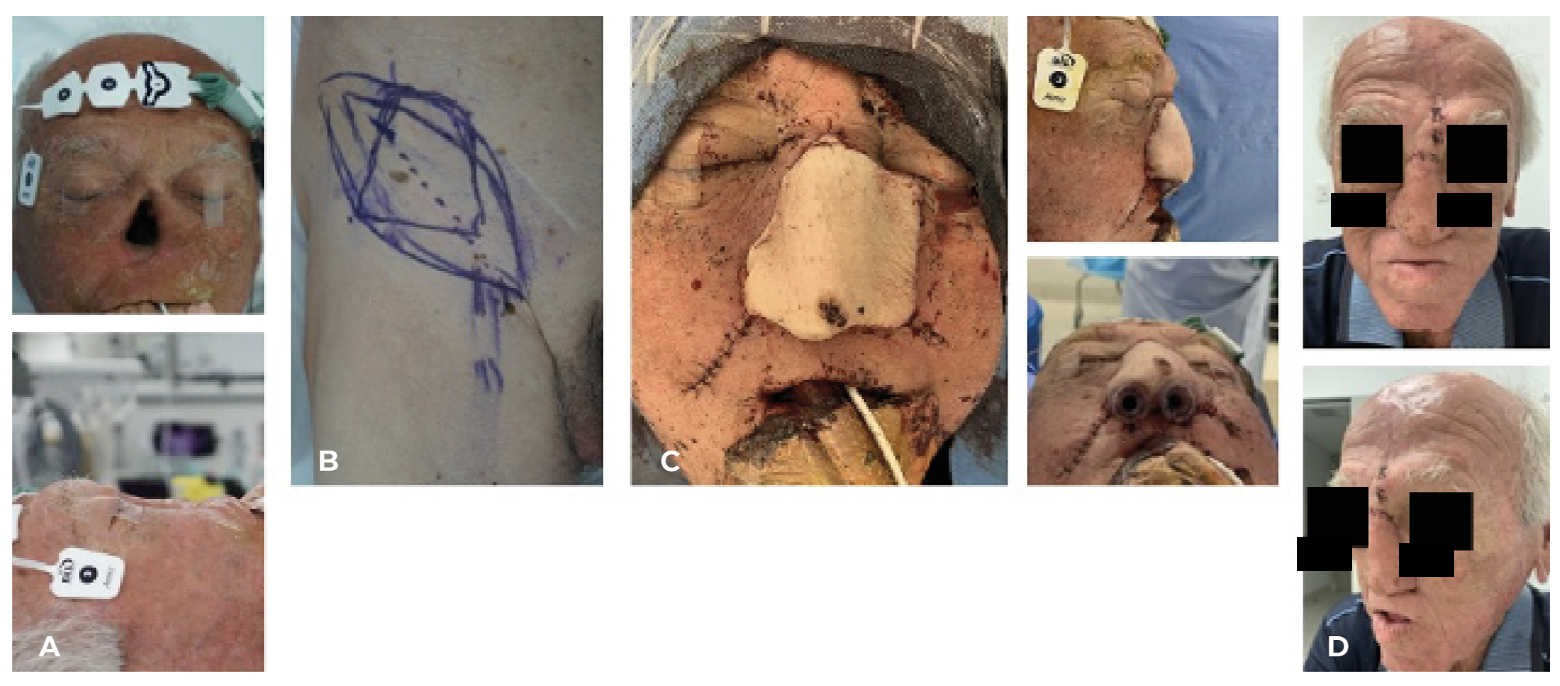
Finally, we employed the novel use of the SCIP flap to provide the nasal lining for a patient undergoing total nasal reconstruction (Figure 6). Multistage nasal reconstruction employing the use of a folded fasciocutaneous flap, typically the radial forearm is a well-established technique popularised by Menick.26 We modified Menick’s technique to utilise the SCIP flap for this purpose, with the added benefit of a more favourable donor site than that of the radial forearm. The flap was designed and inset in a similar fashion to Menick’s radial forearm flap design, incorporating a dorsal cantilever cartilaginous strut covered by the flap. The anastomosis was performed to the facial artery and vein in the nasolabial groove. Unfortunately, the patient was a heavy smoker, and the reconstruction was complicated early by venous congestion resulting in partial flap loss. Adequate tissue was salvaged after an additional vein graft to the superficial temporal vein was performed to allow the flap to provide adequate internal nasal lining, yet the original cantilever strut was lost due to exposure from the flap loss at the dorsal inset. Stage two of the reconstruction was performed three months later, with replacement of the first cantilever strut with a new cartilage graft in L-strut fashion and external coverage with forehead flap. At present follow up the patient is quite pleased with the result.
_total_rhinectomy_de.png)
Conclusion
In our experience, the versatility and adaptability offered by the SCIP flap for a range of different head and neck cancer reconstructions and minimal donor site morbidity suggest that when deployed for the appropriate reconstruction, it is a useful option to consider for the head and neck reconstructive surgeon.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: October 24, 2023 AEST